French and Italian researchers designed a study to improve treatment options for patients with clear-cell renal-cell carcinoma (ccRCC) at intermediate-risk by better characterizing their classification.

A treatment plan for patients with cancer depends acutely on the current stage and progression rate it is discovered in, as well as the type of cancer it is. The more precisely a patients’ risk can be assessed, the more exact their treatment plan can be. This leads directly to better patient outcomes. One way to gauge a patients’ risk is to use a risk-stratified method. Risk stratification is the systematic classification of patients based on the current status of their health and the number of negative clinical prognostic factors that they present with.
From Gustave Roussy, the Gustave Roussy Institute, and the University of Paris-Saclay—each in Villejuif, France—and the University of Modena and Reggio Emilia in Modena, Italy, researchers used a risk-stratified database from the International Metastatic Renal-Cell Carcinoma Database Consortium (IMDC) to carry out a study designed to better characterize intermediate-risk patients with clear-cell renal-cell carcinoma (ccRCC).
The primary goal of the study was to use the information gathered to more precisely tailor treatment for patients with ccRCC in the intermediate-risk classified group. This research paper was chosen as the cover paper of Oncotarget’s Vol 11, Issue #49.
IMDC Risk Stratification Model
The IMDC model of risk stratification uses six negative clinical prognostic factors, including: performance status, hemoglobin level, time between diagnosis and the start of treatment, corrected serum calcium, neutrophil count, and platelet count.
“The International Metastatic renal cell carcinoma Database Consortium (IMDC) score is currently used as a prognostic index to stratify patients with mRCC in three subgroups: good, intermediate and poor-risk groups [1, 2].”
Patients that have three or more of the negative clinical prognostic factors above are considered to be in the poor-risk (of death) outcome group, with the average overall survival estimated at a mere eight months. Patients that present with only one or two of these factors are considered to be in the intermediate-risk group, with the average survival predicted to be approximately 23 months.
Out of 777 patients identified with metastatic ccRCC and treated with an anti-VEGF pathway inhibitor, 51% were classified in the intermediate-risk group. Despite the classification, each of these patients had a different prognosis and the total overall survival was only 27%. Therefore, the researchers argue that patients categorized in the intermediate-risk group should not be treated with the same therapeutic regimen, and designed a study to further categorize this group.
Refining the Intermediate-Risk Classification
Researchers in this study used three approaches to further analyze the intermediate-risk group of patients with metastatic ccRCC in the IMDC risk stratification model and then compared them.
The first approach analyzed the classification based on the number of risk factors patients presented with. They found that the median overall survival was longer by 15 months for patients who presented with only one prognostic factor, as opposed to two. Approach number two analyzed the classification based on a multivariable Cox regression model with backward selection.
“The multivariable Cox model with a backward selection procedure showed that the only prognostic factor associated with OS [overall survival] was platelet count […]”
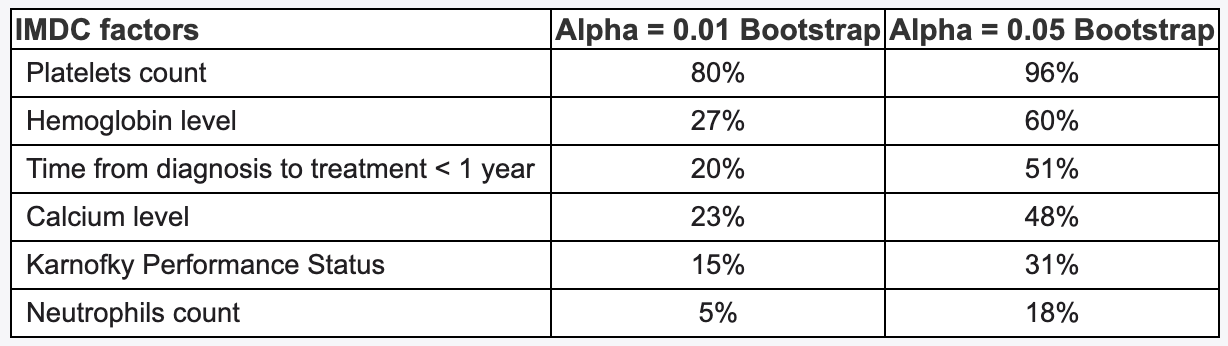
The third approach of analyzing patients with ccRCC in the IMDC intermediate-risk group classification was based on the CART method. The CART-tree analysis clearly identified three separate classes of patients within the intermediate-risk group. CART-tree analysis further categorized patients who had:
- Platelet counts less than or equal to upper normal level, and normal hemoglobin (best prognosis).
- Platelet counts less than or equal to upper normal level, and hemoglobin level less than lower normal level.
- Platelet counts greater than upper normal level (poorest prognosis).
“High platelet count reflecting the cancer-related inflammatory status seems to segregate patients with the worst prognosis in the intermediate-risk group.”
Conclusion
In previous studies, it was demonstrated that platelet aggregation provides multiple survival advantages in tumor cells, including protecting them from immune system defenses. The three approaches of classifying patients with ccRCC in the IMDC model’s intermediate-risk group demonstrated that the patients with higher platelet counts were significantly associated with lower overall survival rates.
Ultimately, three additional subgroups within the IMDC intermediate-risk group were identified. This study may lead to the development of more effective therapeutic options for people living with clear-cell renal-cell carcinoma.
“Further analyses are ongoing to validate these findings in patients receiving first line CPI [checkpoint inhibitor] based combination in first line.”
Click here to read the full scientific paper, published in Oncotarget.
—
Oncotarget is a unique platform designed to house scientific studies in a journal format that is available for anyone to read—without a paywall making access more difficult. This means information that has the potential to benefit our societies from the inside out can be shared with friends, neighbors, colleagues and other researchers, far and wide.
For media inquiries, please contact [email protected].